
An overview of nausea/vomiting in palliative medicine
Abstract: Nausea, vomiting and retching are among the most distressing symptoms that palliative care may experience. This article presents a brief overview of various medical conditions/treatments that may lead to nausea/vomiting/retching as well as potential mechanisms/neurotransmitters/receptors that may be involved and thus may represent therapeutic targets for antiemetic treatments.
Key words: Nausea; vomiting; receptors; chemotherapy-induced nausea/vomiting; radation-induced nausea/ vomiting
Introduction
Smith has defined nausea as an unpleasant sensory and emotional experience which may be described in terms of a “sick” felling with or without a sense of impending vomiting/ retching; often associated with a perception of epigastric or upper abdominal unpleasantness or awareness (1).
The perception of nausea and/or the act of vomiting or retching may be extremely unpleasant and quite severe. Severe nausea, vomiting, or retching can be among the most disabling of symptoms. The patient may suffer an intensely unpleasant and/or distressing experience and some patients may actually choose to live with pain rather than to take a pill that can alleviate their pain if that pill also results in severe nausea. Furthermore, severe nausea, vomiting, and/ or retching may lead to significant adverse effects including: dehydration, electrolyte imbalances, malnutrition, and significant deterioration in quality of life (QOL).
Nausea assessment
Wood and colleagues reviewed various instruments available for the assessment of cancer-related nausea, vomiting, and retching (2). Twenty-four tools evaluating nausea were identified that met their inclusion criteria. Thirteen tools measured vomiting as a separate experience. Only 3 tools included a separate assessment of retching. The number of CINVR-related questions in each tool ranged from 2 to 17 (2).
Of the 24 tools that addressed nausea in the oncology population, many were designed to focus on the patient’s more broad functional status or quality-of-life issues. One commonly used tool, the Morrow Assessment of Nausea and Emesis (3), specifically asked questions regarding pretreatment nausea. Another tool, the MASCC Antiemesis Tool (4), individually addressed both acute and delayed nausea and vomiting.
Rhodes and McDaniel (1999) developed the Index of Nausea, Vomiting, and Retching (INVR) and demonstrated the tool’s ability to be used in both paper and computerized charting (5). The INVR has questions regarding the number of retching episodes in the previous 12 hours and the distress felt by these episodes. The INVR utilizes a 5-point Likerttype scale; although this has not been shown to be as sensitive to early changes as the VAS, it has been found to be clinically useful and easy for patients to understand (2). There have been various versions of this tool published (2). The INVR revised in 1996 addresses the frequency and distress associated with all 3 symptoms: nausea, vomiting, and retching (5).
In 1997, Hesketh et al. classified the acute emetogic potential of individual chemotherapeutic agents (often referred to as the Hesketh score (6). In this system, agents are classified according to proportion of patients expected to experience emesis with each agent in the absence of effective antiemetic prophylaxis as follows: level 1, <10% of patients; level 2, 10-30% of patients; level 3, 30-60% of patients; level 4, 60-90% of patients; and level 5, >90% of patients (6).
Since cisplatin was reported to decrease plasma ghrelin and food intake in rodents, Hiura and colleagues monitored the plasma ghrelin level and its association with nutritional status and adverse events during chemotherapy in patients with esophageal cancer (7). Plasma total ghrelin significantly decreased at days 3 and 8 of chemotherapy and this decrease was associated with a loss of oral intake and appetite (7).
Nausea and vomiting do appear to become more common as death approaches, so it is not surprising that nausea has been found to be a predictor of a shortened survival in one study (8). In patients admitted to specialist palliative care programs, nausea has been reported by 36% patients at the first contact with the service (9-11), 62% at 1-2 months before death (12,13), and 71% in the final week of life (14,15).
Glare and colleagues have categorized nausea etiology in palliative medicine into 4 groups: due to the primary disease, due to a side effect of therapy, secondary to debilitation, and caused by an unrelated comorbid condition for non-medical conditions in palliative medicine associated with nausea mat include significant advanced cardiac obstructive pulmonary disease, end-stage renal disease, and advanced dementia (16).
In elderly palliative care patients, conditions such as mesenteric ischemia, subacute cholangitis, Meniere’s disease, myocardial infarction, drug toxicity, constipation, and urinary tract infection need to be high on the differential diagnosis of nausea and vomiting (16).
Avoidance of environmental stimuli, such as sights, sounds, or smells that may initiate nausea are recommended (17). Fatty, spicy, and highly salted food should be avoided.
Etiologies of nausea/vomiting
There are numerous etiologies for nausea and/or vomiting. Metabolic causes include: uremia, uncontrolled diabetes mellitus, electrolyte imbalance (e.g., sodium, potassium), hormonal imbalance (e.g., hyperemesis gravidarum), altered gastrointestinal tract motility, hyperthyroidism, addison’s disease, and porphyria. Inflammation/irritation/ infection of the airway, posterior pharynx, abdomen (including liver, pancreas, and biliary tree), GI tract, kidneys, bladder, ureter, and testes or cervix may lead to stimulate afferent pathways leading to nausea and/ or vomiting. Additionally, nausea and/or vomiting can result from increased intracranial pressure, chemotherapy, medications/opioids, radiation, movement of endolymph in the semicircular canals-stimulating cranial nerve VIII, hypovolemia/hypotension, pain/anxiety, headaches (e.g., migraine), and unpleasant memories (18). Major causes for nausea/vomiting associated with terminal conditions and the treatment of these conditions include chemotherapyinduced nausea/vomiting (CINV), opioid-induced emesis (OIE), and radiation-induced emesis (RIE).
Chemotherapy-induced nausea and vomiting
The nausea and/or vomiting that occur after chemotherapy are often devastating consequences of cancer treatment. In a survey of oncology patients, Coates et al. reported that nausea and vomiting were the most feared effects of chemotherapy (19). Over a decade later-with the availability of 5-HT3 receptor antagonists-nausea and vomiting remain a top patient fear from chemotherapy (20,21).
Despite advances in antiemetic therapy, 55% of patients receiving highly emetogenic (e.g., cisplatin) chemotherapy experience nausea or vomiting (22) and 41-43% of breast cancer patients receiving moderately emetogenic (e.g., doxorubicin, cyclophosphamide) chemotherapy experience nausea or vomiting (22,23). Additionally, despite standardized treatments and evidence-based guidelines (24-28) (including attempts at creating simpler and more practical tables) (29), 57% of patients administered cisplatin and 36% of patients administered doxorubicin or cyclophosphamide were not treated according to any guidelines in at least one series (22,30). Healthcare providers continue to underestimate the incidence of nausea/vomiting (23) as well as the intensity level of its unpleasantness.
Martin and colleagues designed a new questionnaire to assess the influence of CINV on QOL; due to the lack of a single, standardized, comprehensive questionnaire which assessed the impact of specific components of CINV [also known as chemotherapy-induced nausea and emesis (CINE)] and retching on functioning and well being in the context of cancer-related QOL (31). The new battery style questionnaire used existing scales and items with known psychometric properties including: Functional Assessment of Cancer Therapy (32), European Organization for Research and Treatment of Cancer (EORTC) OLQ-C (30,33) interference of CINV with functioning (the Osoba Nausea and emesis Module) (34), (and the Morrow Assessment of Nausea and Emesis (MANE) (3,31). Additionally, a new retching scale (developed in the format of the MANE) and other new items specific to nausea, emesis, and retching were added to the questionnaire (31).
Chemotherapy can induce acute nausea/vomiting and delayed nausea and vomiting. Delayed emesis can arbitrarily be considered emesis that begins or persists more than 24 hours after chemotherapy. Highly emetogenic therapy may lead to a biphasic pattern of emesis-occurring 2-3 hours after chemotherapy peaking at roughly 6-8 hours, and lasting 10-12 hours following chemotherapy (35).
Delayed emesis may occur in 40-90% of patientsoccurring 18-24 hours post-chemotherapy, peaking at roughly 48-72 hours, and subsiding over the next 2 days (35-37). Therefore, management of CINV for highly emetogenic chemotherapy should be considered over a 5-day period. Moderately emetogenic chemotherapy - induced emesis follows a monophasic pattern-occurring 6-12 hours post-chemotherapy, peaking at about 24 hours, and subsiding 24-36 hours after the administration of chemotherapy (35,38).
Utilizing the European Organization for Research and Treatment in Cancer (EORTC) Quality of Life Questionnaire (QLQ-C30), Rusthoven et al. concluded that patients with CINV after moderately emetogenic chemotherapy experience a significantly negative impact on their health-related quality of life (HRQOL) (39).
Highly emetogenic chemotherapy (e.g., cisplatin) is proposed to evoke serotonin release thereby stimulating 5-HT3 receptors and contributing to CINV (40). Combination of 5-HT3 receptor antagonists with corticosteroids has been advocated as the most effective prophylaxis for CINV (41,42); however, the triple combination of an NK-1 receptor antagonist, a 5-HT3 receptor antagonist, and a corticosteroid may yield optimal efficacy (43). In spite of improvements in CINV with “triple antiemetic therapy” the incidence of CINV remains too high and research efforts to abolish CINV need to continue. Currently, roughly 40-60% of patients continue to experience delayed nausea and vomiting after cisplatin treatment despite combination prophylaxis (dexamethasone with metoclopramide or ondansetron) (35). Kubota and colleagues in a review with meta-analysis concluded that prophylactic treatment with corticosteroids without additional metoclopramide or 5-HT3 receptor antagonists appears preferable for preventing delayed emesis induced by cisplatin, since neither agent demonstrated additional benefits over corticosteroids alone (44).
Opioid-induced emesis (OIE)
Nausea and vomiting are common side effects from opioid therapy-occurring in over 60% of patients (45-47) with nausea being far more common than vomiting. This is generally more of a problem with the initial period of administration of opioids before tolerance to nausea/ vomiting develops. Mechanisms which may contribute to opioid-induced nausea/vomiting include: stimulation of dopamine release in the CTZ/AP, direct opioid receptor stimulation, increased vestibular sensitivity, and impaired GI motility/constipation.
Hirayama et al. found that the best prophylactic antinausea/antiemetic therapy for opioid induced nausea/ vomiting is dexamethasone in doses up to 10mg per day (with an odds ratio of 0.23, 95% confidence interval 0.15-0.35), reducing the incidence of nausea/vomiting from 66-80% to 16-50% (46,47). Once opioid-induced nausea/vomiting is established, 5-HT3 receptor antagonists (“setrons”) may be the best therapy (47-49). Other therapeutic options may include a “setron/steroid” combination or very low doses of opioid receptor antagonists (e.g., naloxone, nalmefene).
Radiation-induced emesis (RIE)
Radiation-induced emesis (RIE) can occur 30 minutes to 4 hours after radiotherapy is delivered and can be prolonged (2-3 days) in up to 40% of patients (50). If RIE is severe enough it can lead to an interruption in the radiotherapy treatment schedule (50,51). Although precise RIE mechanisms remain uncertain, proposed mechanisms include: CTZ/AP stimulation (direct or indirect); stimulation of GI mucosa nerves, neurotransmitter release, direct or indirect stimulation of various “pro-emetic” receptors; cortical or vestibular mechanisms: altered smell/ taste; and/or release of emetic mediators from the tumor area (50). Feyer et al. suggested that serotonin may play a crucial role in RIE-via stimulation of 5-HT3 receptors and in the vagus nerve, greater splanchnic nerves, and CTZ (52).
Yamada et al. suggested that x-ray irradiation activates 5-HT3 receptors on the terminals of abdominal vagal nerves thereby stimulating afferent emetic input to the NTS, leading to increased c-Fos immunoreactivity with subsequent nausea/vomiting (53). Two consensus conferences on antiemetic therapy for RIE-Multinational Association of Supportive Care in Cancer (MASCC) and American Society of Clinical Oncology (ASCO)-support the prophylactic use of 5-HT3 receptor antagonists with or without dexamethadone for patients at high risk for RIE (e.g., total body irradiation) (24,50,51,54).
Pharmacologic treatment strategies for nausea/vomiting
Treatment of nausea/vomiting should be directed at a specific cause if one can be identified. Removing offending agents and correcting etiologies/imbalances that may facilitate nausea/vomiting should constitute initial therapeutic efforts. Targeted therapy (if the cause of nausea/ vomiting is known) is the most rational. Unfortunately, many time clinicians do not know which receptors are most important in contributing to a particular individual’s perception of nausea. The multiple antiemetic agents modulate the actions of one or more receptors (Table 1).
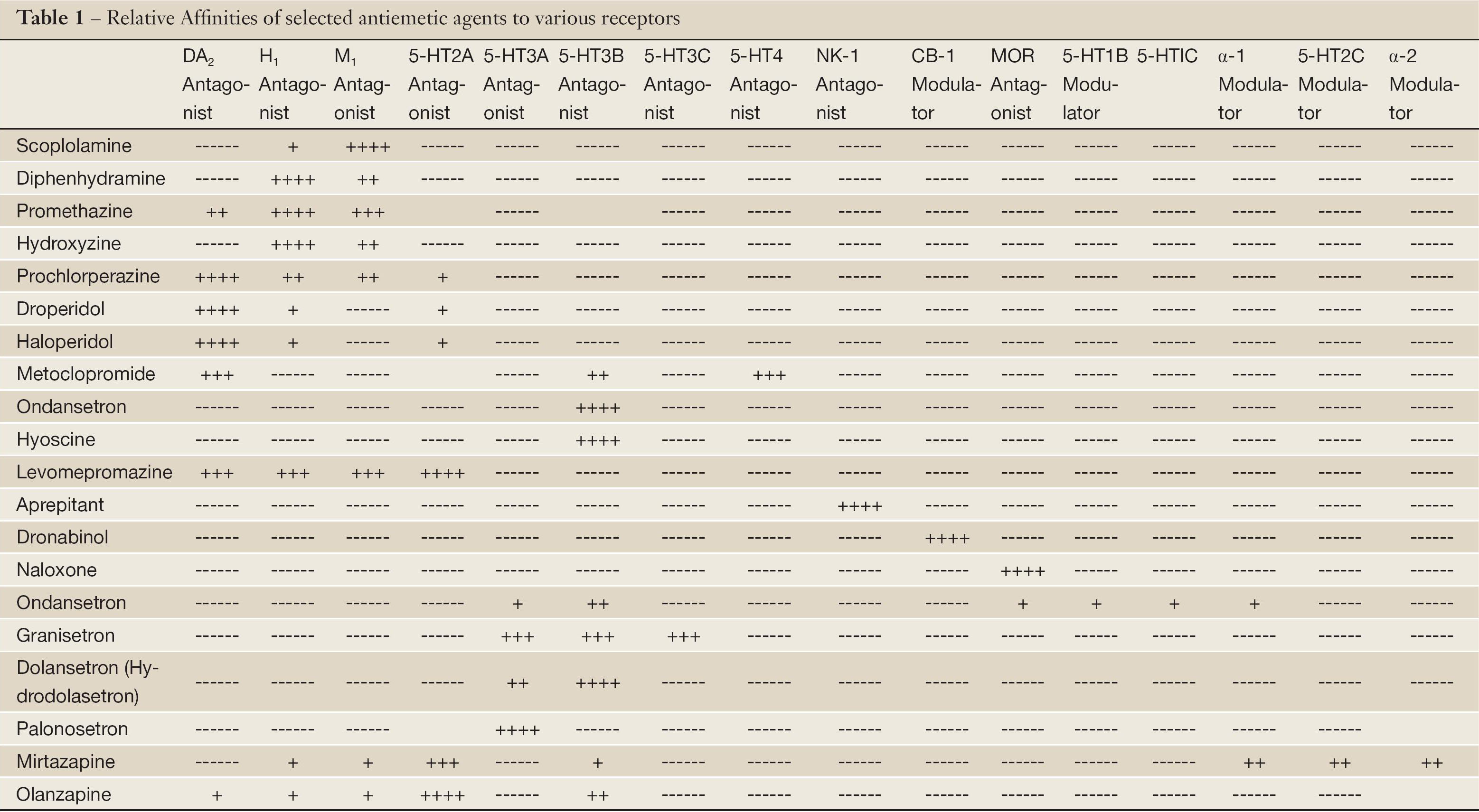
Full table
Commonly used antiemetic drug classes include anticholinergics, antihistamines, sedative/anxiolytics, butyrophenones, phenothiazines, other antidopaminergics, 5-HT3 receptor antagonists, and “glucocorticoid” steroids. The most commonly used anticholinergic agent for prophylaxis of nausea/vomiting is transdermal scopolamine (1.5 mg) patch, which is changed every 3 days. The onset of action of transdermal scopolamine is generally delayed at least 4 hours and it has been used effectively to abort or ameliorate motion-induced vomiting or PONV (55). Side effects of anticholinergic agents include: sedation, dry mouth, blurred vision, mydriasis, urinary retention, hallucinations, central nervous system excitation, memory loss, confusion, and disorientation (55).
Antiemetic agents which are effective for nausea/ vomiting induced by multiple different stimuli may be referred to as broad spectrum antiemetics and antiemetic agents that are effective for nausea/vomiting induced by one specific type of stimulus may be referred to as narrow spectrum antiemetics.
Also, medications which may be effective as prophylactic antiemetics for nausea/vomiting may not be effective for the treatment of nausea and/or vomiting once established. Some antiemetic agents may inhibit emesis but not effectively ameliorate nausea and vice versa, while other antiemetic agents are reasonably effective for combating nausea as well as vomiting.
Additionally, effective therapeutic agents for nausea and/ or vomiting may differ with various specific etiologies. An effective antiemetic for acute chemotherapy-induced emesis may not be effective for the treatment of motion sickness (e.g., 5-HT3 receptor antagonists). Multiple etiologies as well as multiple CNS receptor sites may contribute to nausea and/or vomiting. Therefore, in many cases of nausea and/or vomiting, single drug antiemetic therapy has not been found to provide a complete effective solution. The use of combination therapy and/or a multimodal approach may improve efficacy over monotherapy (56).
The use of rationale polypharmacy in the treatment of nausea and/or vomiting has yielded better results without worsening side effects in combating postoperative nausea and vomiting (18,57-60). A meta-analysis of 26 randomized, controlled studies in 2,561 patients suggested that the addition of dexamethasone to antiemetic monotherapy improved efficacy (61).
If initial monotherapy of nausea/vomiting is only partially effective, clinicians should not change to a different choice of agent (especially if the new agent is an agonist of the same receptor), but rather add an agent to the existing treatment which possesses a different mechanism of action. Additionally, multimodal approaches may include: intravenous hydration, oxygen supplementation, behavioral medicine techniques (62-64), complementary and alternative medicine techniques (including acupuncture/acupressure) (65), and techniques to modulate gastrointestinal motility and/or the vestibular system (18,66).
Phenothiazines block dopaminergic D2 receptors in the CTZ/AP. Heterocyclic phenothiazines (e.g., prochlorperazine) have a piperazine ring at the number 10 portion of the tricyclic nucleus and exhibit more potent antiemetic activity and less sedation than aliphatic phenothiazines (e.g., chlorpromazine, promethazine) but have a higher incidence of extrapyramidal side effects (e.g., tardive dyskinesia, akathesia, acute dystonia, pseudo parkinsonism) (67). Additional side effects which are not rare include dry mouth and hypotension.
The butyrophenones used for nausea/vomiting are droperidol and haloperidol. These agents antagonize dopaminergic D2 receptors at the CTZ/AP and are alpha adrenergic blockers. Side effects may include: hypotension, restlessness, anxiety, dysphoria, sedation, and extrapyramidal symptoms. Droperidol causes a dose-dependent prolongation of the QT interval on the electrocardiogram (68). The United States Food and Drug Administration (FDA) issued a “black box” warning in December 2001 regarding the risk of fatal cardiac arrhythmias (e.g., torsade de pointes) which can occur even with low doses of droperidol (69).
The most commonly used benzamide for nausea/ vomiting is metoclopromide. Metoclopramide is a procainamide derivative with “prokinetic” GI properties which antagonize dopaminergic D2 receptors at the CTZ/AP and peripheral D2 receptors in the GI tract Metoclopramide increases lower esophageal sphincter tone and increases gastric emptying time. Extrapyramidal symptoms can occur but generally at doses higher than 10 mg (70). The repeated use of metoclopramide (especially in higher doses) should be avoided if possible in renal insufficiency and used with great caution in the elderly.
Antihistamines (e.g., hydroxyzine) block acetylcholine in the vestigular system and histamine H1 receptors in the NTS. Common side effects include: dry mouth, sedation, blurred vision, and urinary retention (71).
Benzodiazepines (e.g., lorazepam) have been used to diminish anticipatory nausea and vomiting that may occur before chemotherapy (62). Pharmocologic approaches to anticipatory nausea should probably be used in conjunction with behavioral treatments as well. Steroids (e.g., dexamethasone) are very effective in combination with other agents (e.g., 5HT3 receptor antagonists), however are generally much less impressive as monotherapy.
Glucocorticoids such as dexamethasone are wellestablished antiemetics for chemotherapy-induced as well as postoperative nausea and vomiting. The mechanism of steroid-induced antiemesis remains uncertain but has been assumed to be due to reducing levels of arachidonic acid metabolites that may be emetic (72).
Other explanations advanced have included: inhibition of hypothalamic prostaglandin synthesis, effects on tryptophan depletion, effects on diminished brain levels of serotonin, effects on endorphin release, psychological effects and/ or “membrane-stabilizing” effects (e.g., effects on sodium channel function) (18). The onset time for reasonable antiemetic effects is usually about 4-5 hours (73).
Tetrahydrocannabinol (THC) is more effective than placebo in preventing chemotherapy-induced nausea and vomiting (74). Cannabinoid CB1 receptors in the dorsal vagal complex (75) and NTS (76) may be involved in the nausea-reducing effects of cannabinoids. It appears that cannabinoids not only attenuate vomiting but also play a role in suppressing nausea (77). These effects (in the lithium-induced conditioned rejection reaction rat model of nausea) seem to also be mediated via CB1 receptors since they were reversed by the CB1 receptor antagonist SR-141716A (77). Common side effects of dronabinol (a cannabinoid available for clinical use) are drowsiness, orthostatic hypotension, tachycardia, and dry mouth. Other side effects (especially in the elderly) may include: manic psychoses, depression, anxiety, and visual hallucinations.
Although the mechanisms via which cannabinoids may produce antiemetic effects remains uncertain; potential explanations may include effects on modulation of gastric motility (78), direct effects on cannabinoid receptors located within the “emetic neural circuitry” (79,80) or perhaps by blocking the effects of TNF to amplify vagal afferent responsiveness likely by suppressing neurotransmission by downregulating ryanodine channels through a protein kinase A (PKA)-dependent mechanism (81).
Cannabinoids
At the present time cannabinoids are not recommended as first-line agents for the treatment or prevention of CINV or other N/V states; but may be reserved for patients with intractable N/V unresponsive to other therapies or as rescue for unresponsive breakthrough N/V (82).
The “setrons” (5HT3 receptor antagonists) are relatively effective and reasonably broad spectrum antiemetics that work centrally, blocking the 5HT3 receptor as well as peripherally. These agents are readily absorbed after oral administration and cross the blood-brain barrier without difficulty. The “setrons” are largely metabolized in the liver and have no significant interactions with cytochrome P450 enzyme inducers/inhibitors. Additionally, these agents appear to be relatively free of problems due to drug displacement from binding sites (83). Ondansetron and granisetron are metabolized by CYP3A4-dolasetron and tropisetron are metabolized via CYP2D6 (83). Generally, there is no need to alter dosing in renal insufficiency with conventional dosing (83). However, for patients with significant liver dysfunction a maximal daily dose of 8 mg of ondansetron is recommended (83). The 5HT3 receptor antagonists have a chemical structure that is similar to serotonin. Serotonin has a six-ring carbon structure and a five-ring nitrogen-based nucleus.
The “setron” structures are derived from indole (tropisetron, dolasetron), carbazole (ondensetron), and indazole (granisetron) rings (83). 5HT3 receptor antagonists being investigated include: ramosetron (84), azosetron (18), lerisetron (85), and palonosetron (86,87). Palonosetron exhibits a strong binding affinity to the 5HT3 receptor and a long-plasma elimination half-life (roughly 40 hours) [at least four times greater than other available 5HT3 receptor antagonists] (86,87). Palonosetron may provide effective antiemetic activity for delayed CINV and/or multiple chemotherapy regimens (86,87).
5HT3 receptor antagonists (“setrons”) exhibit a favorable side effect profile. The “setrons” essentially lack the unwanted sedative, extrapyramidal, behavioral, and cardiovascular side effects which other antiemetics may possess (83). Headache and/or lightheadedness/dizziness are not uncommon side effects of the 5HT3 receptor antagonists (83). 5HT3 receptor activation may contribute to the regulation of intestinal propulsive peristalsis and fluid secretion (83,88). High dose “setron” therapy could conceivably slow down intestinal transit, potentially leading to constipation and/or abdominal pain, bloating, or cramping (83,88). Electrocardiogram (ECG) changes of 5HT3 receptor antagonists include: acute asymptomatic, reversible, dose dependent prolongation of the PR, QRS, and QTc intervals (83). Benedict et al. reported a statistically significant increase in QTc interval with the use of intravenous ondansetron and intravenous dolasetron in normal volunteers (89). The Granisetron Transdermal System (GTDS; Sancuso®) (90) may be especially useful in the palliative care population.
NK1 receptor antagonists represent the most recent addition to the pharmacologic therapeutic options aimed at combating nausea/vomiting. The antiemetic activity of NK1 receptor antagonists is largely or entirely from their central action (91). This was demonstrated when Tattersall and colleagues compared 2 different NK1 receptor antagonists.91 L-741, 671, which easily passes through the bloodbrain barrier, demonstrated dose-dependent inhibition of retching/vomiting induced by cisplatin when administered peripherally; however, its quaternary compound L-743,310 (which does not pass through the blood-brain barrier) is inactive when administered peripherally (91,92). When administered centrally both L-741,671 and L-743,310 have equivalent antiemetic activity (91,92).
The five investigational NK1 receptor antagonists studied initially are GR205171 (Glaxo-Wellcome); CP- 122,721 (Pfizer), CJ-11, 974 (Pfizer), L-754-030 (Merck) and its prodrug L-758,298.90 Human studies of the antiemetic qualities of NK1 receptor antagonists have shown effectiveness for cancer chemotherapy-induced nausea and vomiting (CINV) and postoperative nausea and vomiting (PONV) (91,93-98). Patel and Lindley have reviewed the pharmacokinetics and pharmacology of aprepitant (Emend®) which is approved for CINV in the U.S (99).
The Aprepitant Protocol 052 Study Group conducted a multinational, randomized, double-blind, placebo-controlled trial in patients receiving high-dose cisplatin (43). The percentage of patients with complete response on days 1 to 5 was significantly higher in the aprepitant group [72.7% (n=260)] versus the standard therapy group [52.3% (n=260)] as were the percentages on day 1, especially on days 2 to 5 (P<0.001 for all comparisons) (43). They concluded that compared with standard dual therapy (5HT3 receptor antagonist and corticosteroid), addition of aprepitant was generally well tolerated and consistently provided superior protection against CINV (43). Clinicians should be aware that coadministration of aprepitant with dexamethasone or methylprednisolone may result in increased plasma concentrations of the corticosteroids (100). Therefore, adjusting the dose of corticosteroids in this situation may be appropriate.
Fosaprepitant is a prodrug of aprepitant which may be administered intravenously. It is rapidly converted to aprepitant within 30 minutes after the end of infusion. It is indicated for prevention of acute and delayed nausea and vomiting associated with moderaly-and highly-emetogenic chemotherapy (in combination with other anitemetics). The dose is generally 150 mg for first day and 115 mg thereafter. It is administered about a helf-hour prior to chemotherapy as an fision over 20-30 minutes [for 150 mg dose] or over 15 minutes [for 115 mg dose].
Hwang et al. studying the dopamine agonist (-)-N-11Cpropyl- norapomorphine (11C-NPA) in nonhuman primates concluded that 11C-NPA is a suitable (positron emission tomography) PET radiotracer to image/quantify highaffinity sites of dopamine D2-like receptors (101). The high-affinity sites (D2 high) are G protein coupled (101). With the use of these and other techniques (e.g., PET imaging of the CNS utilizing novel radiotracers), it is hoped that insight may be gained into the importance/contribution of the actions of various receptors in facilitating nausea/ vomiting in an individual patient. In the future, armed with this knowledge, clinicians may be able to design optimal antiemetic “cocktails” for individual patients.
Nonpharmacologic treatment strategies for nause/vomiting
Gastric electrical stimulation (GES) has been introduced for treating gastric motility disorders. GES with long pulses or dual pulses, but not short pulses, are able to alter (enhance or inhibit) such parameters of gastric motility as gastric slow waves and gastric emptying. Synchronized GES has been reported to improve antral contractions. A special method of GES using high frequency-short pulses, called Enterra® Therapy, has been clinically applied to treat nausea and vomiting in patients with gastroparesis (102). Although the mechanisms of gastric electrical stimulation remain uncertain, improved gastric accommodation, direct enteric nervous system effects, enhanced vagal activity, and activation of central neurons are believed to be the underlying mechanisms involved in the antiemetic effect of Enterra® therapy (102).
Although the literature is scant and results have been mixed, behavioral approaches such as relaxation and distraction, relaxation training utilizing muscle relaxation and guided imagery. Massage has been reported to be effective for nausea and pain in bone marrow transplant patients (103). Foot massage was shown to reduce nausea significantly in hospitalized cancer patients (104). A systematic review of complementary and alternative medicine for symptom management at the end of life was unable to identify any large-scale trials in terminally ill patients for nausea and vomiting.
Acupuncture has been fairly well established in the prevention of PONV (105). It consists of stimulating the so-called P6 wrist point (located on the ventral surface of the forearm approximately 3 fingerwidths proximal to the wrist joint) by using acupuncture, acupressure, and other techniques (106). Acupuncture and ginger have been shown to be effective for chemotherapy-induced emesis and anticipatory nausea (107,108), but have not been evaluated in the nausea of far advanced disease.
Summary
Nausea, vomiting and retching are among the worst of symptoms that patients may experience. Despite the existence of evaluation and management guidelines as well as many antiemetic agents, the clinical results of the treatment of nausea, vomiting and retching remain suboptimal. A greater appreciation of the neurotransmitters/ mediators that may contribute to nausea, vomiting, and retching in an individual patient, as well as the specific receptors/receptor subtypes where they act, will hopefully lead to improved patient outcomes.
Acknowledgements
The author would like to thank Pya Seidner for her enormous assistance in the preparation of this manuscript.
Disclosure: The authors declare no conflict of interest.
References
- Smith HS. A receptor-based paradigm of nausea and vomiting. Journal of Cancer Pain and Symptom Palliation 2005;1:11-23.
- Wood JM, Chapman K, Eilers J. Tools for assessing nausea, vomiting, and retching. Cancer Nurs 2011;34:E14-24.
- Morrow GR. The assessment of nausea and vomiting: past problems, current issues, and suggestions for future research. Cancer 1984;53:2267-80.
- MASCC Antiemesis Tool (MAT). Available online: http://www.mascc.org/index.php?option=com_ content&view=article&id=143. Accessed 2012.
- Rhodes VA, McDaniel RW. The Index of Nausea, Vomiting, and Retching: a new format of the Index of Nausea and Vomiting. Oncol Nurs Forum 1999;26:889-94.
- Hesketh PJ, Kris MG, Grunberg SM, et al. Proposal for classifying the acute emetogenicity of cancer chemotherapy. J Clin Oncol 1997;15:103-9.
- Hiura Y, Takiguchi S, Yamamoto K, et al. Fall in plasma ghrelin concentrations after cisplatin-based chemotherapy in esophageal cancer patients. Int J Clin Oncol 2012;17:316-23.
- Chang VT, Hwang SS, Kasimis B, et al. Shorter symptom assessment instruments: the Condensed Memorial Symptom Assessment Scale (CMSAS). Cancer Invest 2004;22:526-36.
- Ventafridda V, De Conno F, Ripamonti C, et al. Qualityof- life assessment during a palliative care programme. Ann Oncol 1990;1:415-20.
- Donnelly S, Walsh D, Rybicki L. The symptoms of advanced cancer: identification of clinical and research priorities by assessment of prevalence and severity. J Palliat Care 1995;11:27-32.
- Vainio A, Auvinen A. Prevalence of symptoms among patients with advanced cancer: an international collaborative study. Symptom Prevalence Group. J Pain Symptom Manage 1996;12:3-10.
- Reuben DB, Mor V. Nausea and vomiting in terminal cancer patients. Arch Intern Med 1986;146:2021-3.
- Coyle N, Adelhardt J, Foley KM, et al. Character of terminal illness in the advanced cancer patient: pain and other symptoms during the last four weeks of life. J Pain Symptom Manage 1990;5:83-93.
- Fainsinger R, Miller MJ, Bruera E, et al. Symptom control during the last week of life on a palliative care unit. J Palliat Care 1991;7:5-11.
- Conill C, Verger E, Henriquez I, et al. Symptom prevalence in the last week of life. J Pain Symptom Manage 1997;14:328-31.
- Glare P, Miller J, Nikolova T, et al. Treating nausea and vomiting in palliative care: a review. Clin Interv Aging 2011;6:243-59.
- Rhodes VA, McDaniel RW. Nausea, vomiting, and retching: complex problems in palliative care. CA Cancer J Clin 2001;51:232-48.
- Kovac AL. Prevention and Treatment of Postoperative Nausea and Vomiting. In: Donnerer J, ed. Switzerland: Antiemetic Therapy. S. Karger AG. Basel, 2003:121-60.
- Coates A, Abraham S, Kaye SB, et al. On the receiving end: Patient perception of the side effects of cancer chemotherapy. Eur J Cancer Clin Oncol 1983;19:203-8.
- Griffin AM, Butow PN, Coates AS, et al. On the receiving end V: Patient perceptions of the side effects of cancer chemotherapy in 1993. Ann Oncol 1996;7:189-95.
- de Boer-Dennert M, de Wit R, Schmitz PI. Patient perceptions of the side effects of chemotherapy: The influence of 5 HT3 antagonists. Br J Cancer 1997;76:1055-61.
- Fabi A, Barduagni M, Lauro S, et al. Is delayed chemotherapy-induced emesis well managed in oncological clinical practice: An observational study. Support Care Cancer 2003;11:156-61.
- Grunberg SM, Hansen M, Deuson R, et al. Incidence and impact of nausea/vomiting with modern antiemetic: Perception vs. reality. Proc Am Soc Clin Oncol 2002;21:250 (abstr 996).
- Gralla RJ, Osoba D, Kris MG, et al. Clinical practice guidelines for the use of antiemetics: Evidence-based report by the American society of Clinical Oncology. J Clin Oncol 1999;17:2971-94.
- Osoba D, Warr D, Fitch M, et al. Guidelines for the optimal management of chemotherapy-induced nausea and vomiting: A consensus. Can J Oncol 1995;5:381-400.
- NCCN antiemesis practice guidelines. Oncology 1997;11:57-89.
- American Society of Health-System Pharmacists: ASHP therapeutic guidelines on the pharmacologic management of nausea and vomiting in adult and pediatric patients receiving chemotherapy or radiation therapy or undergoing surgery. Am J Health Sys Pharm 1999;56:729-64.
- Roila F, Del Favero A, Gralla RJ, et al. Prevention of chemotherapy-and radiotherapy-induced emesis: Results of the Perugia Consensus Conference. Ann Oncol 1998;9:811-9.
- Koeller JM, Aapro MS, Gralla RJ, et al. Antiemetic guidelines: creating a more practical treatment approach. Support Care Cancer 2002;10:519-22.
- Kris MG. Why do we need another antiemetic? Just ask. J Clin Oncol 2003;21:4077-80.
- Martin CG, Rubensten EB, Elting LS, et al. Measuring chemotherapy-induced nausea and emesis. Psychometric properties of a quality of life questionnaire. Cancer 2003;98:645-55.
- Cella DF, Tulsky DS, Gray G, et al. The functional Assessment of Cancer Therapy Scale: development and validation of the general measure. J Clin Oncol 1993;11:570-9.
- Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-30: a quality-of-life instrument for use in international trials in oncology. J Natl Cancer Inst 1993;85:365-76.
- Osoba D, Zee B, Warr D, et al. Effect of post chemotherapy nausea and vomiting on health-related quality of life. Support Care Cancer 1997;5:307-13.
- Roila F. Prevention of Delayed Nausea and Emesis Induced by Chemotherapy. In: Donnerer J, ed. Switzerland: Antiemetic Therapy. S. Karger AG. Basel, 2003:169-78.
- Gralla RJ, Itri LM, Pisko SE, et al. Antiemetic efficacy of high-dose metoclopramide: Randomized trials with placebo and prochlorperazine in patients with chemotherapy-induced nausea and vomiting. N Engl J Med 1981;305:905-9.
- Kris MG, Gralla RJ, Clark RA, et al. Incidence, course and severity of delayed nausea and vomiting following the administration of high-dose cisplatin. J Clin Oncol 1985;3:1379-84.
- Martin M. The severity and pattern of emesis following different cytotoxic agents. Oncology 1996;53:26-31.
- Rusthoven JJ, Osoba D, Butts CVA, et al. The impact of post chemotherapy nausea and vomiting on quality of life after moderately emetogenic chemotherapy. Support Care Cancer 1998;6:389-95.
- Minami M, Edno T, Hirafuji M, et al. Pharmacological aspects of anticancer drug-induced emesis with emphasis on serotonin release and vagal nerve activity. Pharmacol Ther 2003;99:149-65.
- The Italian Group for Antiemetic Research: Dexamethasone alone or in combination with ondansetron for the prevention of delayed nausea and vomiting induced by chemotherapy. N Engl J Med 2000;342:1554-9.
- Roila F, Tonato M, Cognetti F, et al. Prevention of cisplatin-induced emesis: a double-blind multicenter randomized crossover study comparing ondansetron and ondansetron plus dexamethasone. J Clin Oncol 1991;9:675-8.
- Hesketh PJ, Grunberg SM, Gralla RJ, et al. The oral neurokinin-1 antagonist aprepitant for the prevention of chemotherapy-induced nausea and vomiting: a multinational, randomized double-blind, placebocontrolled trial in patients receiving high-dose cisplatinthe Aprepitant Protocol 052 Study Group. J Clin Oncol 2003;21:4112-9.
- Kubota Y, Mihara K, Ishii F, et al. Effectiveness of antiemetics for the prophylaxis of cisplatin-induced delayed emesis: a systematic review. Yakugaku Zasshi 2004;124:1-11.
- Tramèr MR, Walder B. Efficacy and adverse effects of prophylactic antiemetics during patient-controlled analgesia therapy: A quantitative systematic review. Anesth Analg 1999;88:1354-61.
- Hirayama T, Ishii F, Yago K, et al. Evaluation of the effective drugs for the prevention of nausea and vomiting induced by morphine used for postoperative pain: A quantitative systematic review. Yakugaku Zasshi 2001;121:179-85.
- Aparasu RR, Aparasu A. Management of Opioid-induced Nausea of emesis. In: Donnerer J, ed. Switzerland: Antiemetic Therapy. S. Karger AG. Basel, 2003:113-20.
- Sussman G, Shurman J, Creed MR, et al. Intravenous ondansetron for the control of opioid-induced nausea and vomiting. International S3AA3013 Study Group. Clin Ther 1999;21:1216-27.
- Chung F, Lane R, Spraggs C, et al. Ondansetron is more effective than metoclopramide for the treatment of opioid-induced emesis in post-surgical adult patients. Ondansetron OIE Post-Surgical Study Group. Eur J Anaesthesiol 1999;16:669-77.
- Maranzano E. Prophylaxis of Radiation-Induced Emesis. In: Donnerer J, ed. Switzerland: Antiemetic Therapy. S. Karger AG. Basel, 2003:179-91.
- Tonini G, Vincenzi B, Santini D, et al. Prevention of radiotherapy-induced emesis. J Exp Clin Cancer Res 2003;22:17-22.
- Feyer PC, Stewart AL, Titlbach OJ. Aetiology and prevention of emesis induced by radiotherapy. Support Care Cancer 1998;6:253-60.
- Yamada Y, Tsukamoto G, Kobashi M, et al. Abdominal Vagi mediate c-Fos expression induced by x-ray irradiation in the nucleus tractus solitarii of the rat. Auton Neurosci 2000;83:29-36.
- Antiemetic Subcommittee of the Multinational Association of Supportive Carc in Cancer Consensus Conference. (MASCC). Prevention of chemotherapy and radiotherapyinduced emesis. Results of the Perugia Consensus Conference. Ann Oncol 1998;9:811-9.
- Bailey PL, Streisand JB, Pace NL, et al. Transdermal scopolamine reduces nausea and vomiting after outpatient laparoscopy. Anesthesiology 1990;72:977-80.
- Scuderi PE, James RL, Harris L, et al. Multimodal management prevents early postoperative vomiting after out-patient laparoscopy. Anesth Analg 2000;91:1408-14.
- McKenzie R, Tantisira B, Karambelker DJ, et al. Comparison of ondansetron with ondansetron plus dexamethasone in the prevention of postoperative nausea and vomiting. Anesth Analg 1994;79:961-4.
- McKenzie R, Uy NTL, Riley TJ, et al. Droperidol/ Ondansetron combination controls nausea and vomiting after tubal bonding. Anesth Analg 1996;83:1218-22.
- Fujii Y, Toyook H, Tanaka H. Prevention of postoperative nausea and vomiting with a combination of granisetron and droperidol. Anesth Analg 1998;86:613-6.
- Fujii Y, Tanaka H, Toyooka H, et al. Granisetrondesamethasone combination reduces postoperative nausea and vomiting. Can J Anaesth 1995;42:387-90.
- Eberhart LH, Morin AM, Georgieff M. Dexamethasone for prophylaxis of postoperative nausea and vomiting. A meta-analysis of randomized controlled studies. Anaesthesist 2000;49:713-20.
- Morrow GR, Morrell C. Behavioral treatment for the anticipatory nausea and vomiting induced by cancer chemotherapy. N Engl J Med 1982;307:1476-80.
- Genuis ML. The use of hypnosis in helping cancer patients control anxiety, pain and emesis: A review of recent empirical studies. Am J Clin Hypn 1995;37:316-25.
- Latimer PR, Malmud LS, Fisher RS. Gastric stasis and vomiting: behavioral treatment. Gastroenterology 1982;83:684-8.
- Harmon D, Ryan M, Kelly A, et al. Acupressure and prevention of nausea and vomiting during and after spinal anesthesia for caesarean section. Br J Anaesth 2000;84:463-7.
- Lee A, Done ML. The use of nonpharmacologic techniques to prevent postoperative nausea and vomiting: a meta-analysis. Anesth Analg 1999;88:1362-9.
- Dundee JW, Assaf FAE, Loan WB, et al. A comparison of the efficacy of cyclizine and perphenazine in reducing the emetic effects of morphine and pethidine. Br J Clin Pharmacol 1975;2:81-5.
- Lischke V, BehneM, Doelken P, et al. Droperidol causes a dose-dependent prolongation of the QT interval. Anesth Analg 1994;79:983-6.
- FDA strengthens warnings for droperidol. Available online: http://www.fda.gov/ohrms/dockets/ac/03/ briefing/4000B1_05_FDA%20Talk%20Paper%2012-05- 01.pdf . Accessed 2012.
- Kauste A, Tuominen M, Heikkinen H, et al. Droperidol, alizapride and metoclopramide in the prevention and treatment of postoperative emetic sequelae. Eur J Anaesth 1986;3:1-9.
- Bellville JW, Howland WS, Bross ID. Postoperative nausea and vomiting. III. Evaluation of the antiemetic drugs fluphenazine (prolixin) and promethazine (phenergan) and comparison with triflupormazine (vesprin) and cyclizine (marczine). J Am Med Assoc 1960;172:1488-93.
- Becker DE. Nausea, vomiting, and hiccups: a review of mechanisms and treatment. Anesth Prog. 2010;57:150-6.
- Henzi I, Walder B, Tramer MR. Dexamethasone for the prevention of postoperative nausea and vomiting: A qualitative systemic review. Anesth Analg 2000;90:186-94.
- Wadibia EC. Antiemetics. South Med J 1999;92:162-5.
- Hornby, PJ. Central neurocircuitry associated with emesis. Am J Med 2001;111:106S-12S.
- Himmi T, Dallaporta M, Perrin J, et al. Neuronal responses to delta 9-tetrahydrocannabinol in the solitary tract nucleus. Eur J Pharmacol 1996;312:273-9.
- Parker LA, Mechoulam R, Schlievert C, et al. Effects of cannabinoids on lithium-induced conditioned rejection reaction in a rat model of nausea. Psychopharmacology (Berl) 2003;166:156-62.
- Abalo R, Vera G, López-Pérez AE, et al. The Gastrointestinal Pharmacology of Cannabinoids: Focus on Motility. Pharmacology 2012;90:1-10.
- Martin BR, Wiley JL. Mechanism of action of cannabinoids: how it may lead to treatment of cachexia, emesis, and pain. J Support Oncol 2004;2:305-14; discussion 314-6.
- Walsh D, Nelson KA, Mahmoud FA. Established and potential therapeutic applications of cannabinoids in oncology. Support Care Cancer 2003;11:137-43.
- Rogers RC, Hermann GE. Tumor necrosis factor activation of vagal afferent terminal calcium is blocked by cannabinoids. J Neurosci 2012;32:5237-41.
- Todaro B. Cannabinoids in the treatment of chemotherapy-induced nausea and vomiting. J Natl Compr Canc Netw 2012;10:487-92.
- Donnerer J, Beubler E. 5-HT3 Receptor Antagonists in Antiemetic Therapy. In: Donnerer J. ed. Switzerland: Antiemetic Therapy. S. Karger AG. Basel, 2003:22-32.
- Villalon A, Chan V. Multicenter, randomized trial of ramosetron plus dexamethasone versus ramosetron alone in controlling cisplatin-induced emesis. Support Care Cancer 2004;12:58-63.
- Huckle R. Lerisetron. FAES. Curr Opin Investig Drugs 2003;4:874-7.
- Eisenberg P, Figueron-Vadillo J, Zamora R, et al. Improved prevention of moderately emetogenic chemotherapy-induced nausea and vomiting with palonosetron, a pharmacologically novel 5-HT3 receptor antagonist: results of a phase III, single-dose trial versus dolasetron. Cancer 2003;98:2473-82.
- Grunberg SM, Koeller JM. Palonosetron: a unique 5-HT3-receptor antagonist for the prevention of chemotherapy-induced emesis. Expert Opin Pharmacother 2003;4:2297-303.
- Haga K, Asano K, Fukuda T, et al. The function of 5-HT3 receptors on colonic transit in rats. Obes Res 1995;3:801S-10S.
- Benedict CR, Arbogast R, Martin L, et al. Single-blind study of the effects of intravenous dolansetron mesylate versus ondansetron on electrocardiographic parameters in normal volunteers. J Cardiovasc Pharmacol 1996;28:53-9.
- Boccia RV, Clark G, Howell JD. Use of trandermal and intravenous granisetron and the ability of the Hesketh score to assess nausea and vomiting induced by multiday chemotherapy. Cancer Manag Res 2012;4:171-6.
- Diemunsch P, Grelot L. Potential of Substance P Antagonists as antiemetics. In: Donnerer J, ed. Switzerland: Antiemetic Therapy. S. Karger AG. Basel, 2003:78-97.
- Tattersall FD, Rycroft W, Francis B, et al. Tachykinin NK1 receptor antagonists act centrally to inhibit emesis induced by the chemotherapeutic agent cisplatin in ferrets. Neuropharmacology 1996;35:1121-9.
- Cocquyt V, VanBelle S, Reinhardt RR, et al. Comparison of L-758,298, a prodrug for the selective neurokinin-1 antagonist, L-754,030, with ondansetron for the prevention of cis-platin-induced emesis. Eur J Cancer 2001;37:835-42.
- Navari RM, Reinhardt RR, Gralla RJ, et al. Reduction of cisplatin-induced emesis by a selective neurokinin-1 receptor antagonist. N Engl J Med 1999;340:190-5.
- Campos D, Pereira JR, Reinhardt RR, et al. Prevention of cisplatin-induced emesis by the oral neurokinin-1 antagonist, MK-869, in combination with granisetron and dexamethasone or with dexamethasone alone. J Clin Oncol 2001;19:1759-67.
- Gesztesi Z, Scuderi PE, White PF, et al. Substance P (neurokinin-1) antagonist prevents postoperative vomiting after abdominal hysterectomy procedures. Anesthesiology 2000;93:931-7.
- Diemunsch P, Schoeffler P, Bryssine B, et al. Anti-emetic activity of the NK1 receptor antagonist GR205171 in the treatment of established PONV following major gynecological surgery. Br J Anaesth 1999;82:274-6.
- Hesketh PJ, Gralla RJ, Webb RT, et al. Randomized phase II study of the neurokinin-1 receptor antagonist CJ-11,974 in the control of cisplatin-induced emesis. J Clin Oncol 1999;17:338-43.
- Patel L, Lindley C. Aprepitant-a novel NK1-receptor antagonist. Expert Opin Pharmaco Ther 2003;4:2279-96.
- McCrea JB, Majumdar AK, Goldberg MR, et al. Effects of the neurokinin 1 receptor antagonist aprepitant on the pharmacokinetics of dexamethasone and methylprednisolone. Clin Pharmacol Ther 2003;74:17-24.
- Hwang D-R, Narendran R, Huang Y, et al. Quantitative analysis of(-)-N-11C-Propyl-Norapomorphine in vivo binding in nonhuman primates. J Nucl Med 2004;45:338-46.
- Yin J, Abell TD, McCallum RW, et al. Gastric neuromodulation with enterra system for nausea and vomiting in patients with gastroparesis. Neuromodulation 2012;15:224-31.
- Ahles TA, Tope DM, Pinkson B, et al. Massage therapy for patients undergoing autologous bone marrow transplantation. J Pain Symptom Manage 1999;18:157-63.
- Grealish L, Lomasney A, Whiteman B. Foot massage. A nursing intervention to modify the distressing symptoms of pain and nausea in patients hospitalized with cancer. Cancer Nurs 2000;23:237-43.
- Lee A, Fan LT. Stimulation of the wrist acupuncture point P6 for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev 2009;2:CD003281.
- Chernyak GV, Sessler DI. Perioperative acupuncture and related techniques. Anesthesiology 2005;102:1031-49.
- Ezzo JM, Richardson MA, Vickers A, et al. Acupuncturepoint stimulation for chemotherapy-induced nausea or vomiting. Cochrane Database Syst Rev 2006;2:CD002285.
- Hickok JT, Roscoe JA, Morrow GR, et al. A Phase II/ III randomized, placebo-controlled, double-blind clinical trial of ginger (Zingiber officinale) for nausea caused by chemotherapy for cancer: a currently accruing URCC CCOP Cancer Control Study. Support Cancer Ther 2007;4:247-50.

